
PHILADELPHIA — She called it her “deepest, darkest secret,” one she had never even shared with her husband. When Saffiatu Sillah was growing up in the West African nation of Sierra Leone, her clitoris was cut off in a ritual circumcision.
She was left with scar tissue that caused pain during sex and agony during childbirth. After her second child was born, Ms. Sillah, a pharmacist then living in Philadelphia, searched for medical help. Dr. Ivona Percec, a plastic surgeon at the University of Pennsylvania, said she thought an operation could ease the pain but might fail to uncover any remnant of the clitoris beneath the scarring.
“There might not be anything left,” Dr. Percec cautioned. But she was willing to try. “It’s like digging for buried treasure. Everyone thinks it’s just the little triangle that protrudes. That’s just the tip of it.”
More than 200 million women and girls alive today have undergone genital cutting in 30 countries in Africa, the Middle East and Asia, ranging from nicks to extreme damage. Yet despite the extraordinary need for appropriate medical care, there has been little rigorous research on how surgeons can relieveenduring physical harm or improve sexual sensation.
“They come to us seeking solutions that will optimize their health — both physical and psychosexual,” said Dr. Nawal M. Nour, an obstetrician-gynecologist who directs the African Women’s Health Center at Brigham and Women’s Hospital in Boston. “Presently, we are failing them because we lack the research that can guarantee their best outcome.”
With Ms. Sillah’s operation in 2016, Dr. Percec joined a small but growing number of doctors worldwide performing such surgeries.
The procedure, often called clitoral reconstruction or restoration, is viewed with caution and skepticism by some medical experts. The World Health Organization says that while there are some promising reports that the operation may relieve pain, there is not yet enough evidence of safety and effectiveness. The organization advises against raising unrealistic expectations, especially for women seeking sexual improvement.
Still, demand for such operations is growing in the United States and other Western nations as more women who have been genitally cut move to countries where medical techniques are advanced, insurance often covers surgery, and women can make decisions about their bodies.
Over the past two years, four women — a health professional, a hairstylist, a bus driver and Ms. Sillah, the hospital pharmacist — shared intimate details of their experiences, and one allowed me to be in the operating room during her surgery. They described physical and emotional traumas, struggles with ruined relationships and feelings of shame that they were not “normal.”
All were patients of Dr. Percec (pronounced per-check). She regularly performs plastic surgery for medical or cosmetic reasons, including labiaplasty to reshape the inner labia, but until Ms. Sillah contacted her, she had never tried clitoral reconstruction on women who were cut.

Her most complex patient so far is a health professional from Sudan, where 87 percent of women have been cut. Like many Sudanese women, this patient underwent the most extreme form called infibulation: Clitoris, labia majora and minora are severed, labia are repositioned and the vagina is sewn mostly closed, requiring surgical opening for childbirth. Infibulation makes urination, menstruation and sex arduous, and increases risks of pregnancy complications.
The 30-year-old patient, who asked to be identified only by her initials, S.A., because relatives in Sudan were unaware of her 2017 surgery, said she was infibulated at age 9. She was told that it was needed to reduce sexual sensation and prevent promiscuity, and that “when you become tight, your husband will love you more.”
In her 20s, she married a Sudanese-American man she met via Facebook. Her husband, A.A., 37, said he was determined to be sensitive about her discomfort so she could “be enjoying her wedding night without being scared.” Still, she said, for a while, sex hurt. She never had an orgasm.
After she joined him in Pennsylvania, he encouraged her search for clitoral reconstruction. “My God, that place is really sewn up; how’s the baby going to come out?” he wondered.
Dr. Percec cut through S.A.’s stitching and scar tissue, removed a large uncomfortable cyst that resulted from the circumcision, widened the vaginal opening and surfaced the remaining clitoris.
S.A. so appreciated her new anatomy that she frequently looked at it with a mirror. After weeks of recovery she felt more sensation, and intercourse became more comfortable.
“It was so tight,” said S.A., who has since given birth without complications. “Now, relations are much better.”
“Yes, yes, yes, 600 percent,” her husband agreed. “There is a lot of change, not only from her side, but from my side because she gained confidence in herself, and now she’s more natural.”
For Ms. Sillah, the trauma of circumcision began at age 7, when she was blindfolded and cut, causing “the most excruciating pain.” She was told, “This is what makes you a woman.” As her wound healed, her labia fused together, leaving a narrow opening.
After joining her mother in New Jersey at 16, she held off on dating, fearing men would be appalled. When she finally had sex, she said, “it was so painful.”
Two grueling childbirths drove her to seek surgery.
Dr. Percec counseled Ms. Sillah, now 36, to inform her husband, Mtijan Kamara, about the operation — an emotionally difficult request because Ms. Sillah had told him before they married that she had not been cut. Although he was also from Sierra Leone, he was raised to oppose cutting. She had worried he would think less of her.
Nervously, she disclosed the truth.
“You sure?” he replied, surprised because, unlike some women who have been cut, she experienced sexual pleasure. He comforted her, saying, “You’re fine, leave it as it is.” But because she feared pain with future pregnancies, he supported her choice.
After she awoke from surgery, Dr. Percec announced remarkable news: “I found your clitoris!”
Ms. Sillah said she felt complete as a woman for the first time.
“Like wow — I actually have a clitoris sitting there,” said Ms. Sillah, who now lives in Maryland. “I always had an orgasm but, oh my gosh, it’s so much better.”
Mixed evidence, growing demand
Genital cutting, also called female genital mutilation, is a centuries-old practice that varies by culture. International efforts to end cutting have been somewhat successful, but it persists in many countries. It often involves severing a girl’s visible clitoris, while the rest, several centimeters or more, remains beneath the surface.
One pioneer of surgery to counteract the effects of genital cutting is Dr. Pierre Foldès, a French urologist, who helped found a humanitarian organization, Doctors of the World. He realized that the uncut clitoris was sealed underneath scar tissue, often pushed back and up, adhering to the pubic bone. He devised a technique to unearth the clitoral remnant and shift it into position by detaching connective tissue called a suspensory ligament.
He says he has operated on about 6,000 women, mostly in France, and trained about 200 surgeons, primarily in Africa.
He led the largest, most comprehensive study of clitoral reconstruction, involving 2,938 women from 1998 to 2009, although the study had significant limitations, including that he assessed his own work.
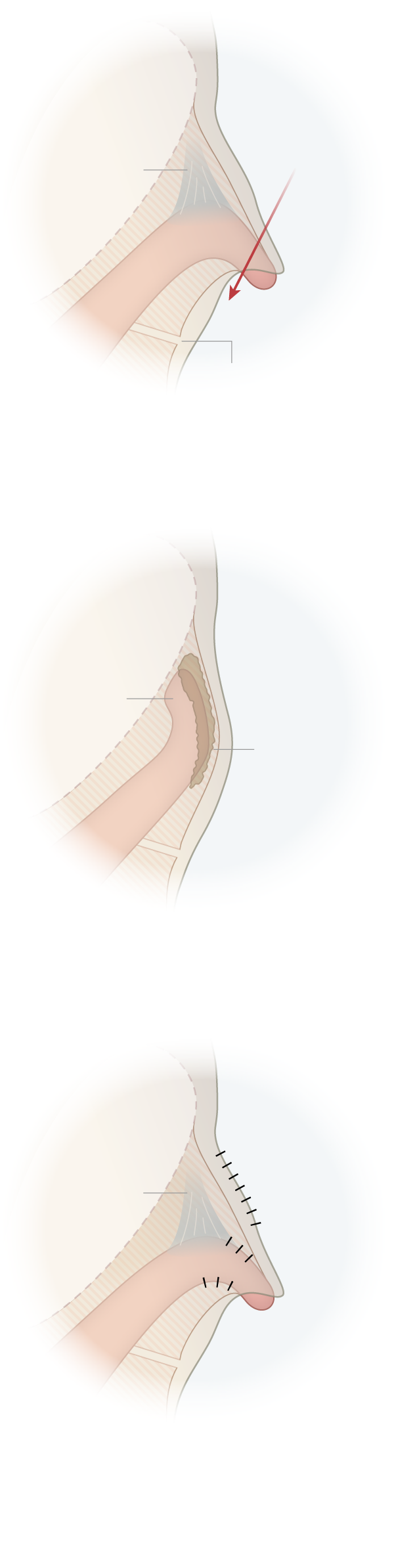
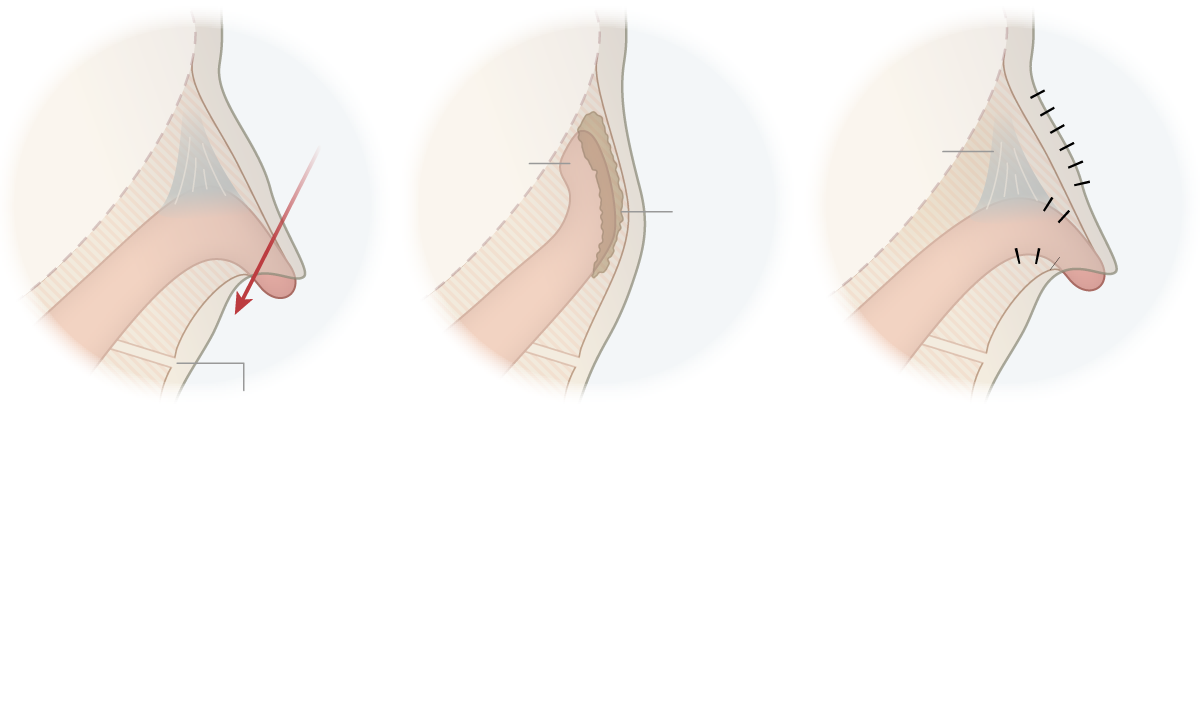
Reconstructive Surgery
Surgeons have developed techniques to restore the clitoris after genital cutting.
Pubic
bone
Cut
Suspensory
ligament
Clitoral
hood
Clitoral
body
Glans
clitoris
Urethra
GENITAL CUTTING
Several types of female genital cutting include the removal or cutting of the glans clitoris, the visible or palpable tip of the clitoris.
Pubic
bone
Clitoral
remnant
Scar
tissue
SCAR TISSUE
As it heals, the clitoral remnant can become buried by scar tissue and stuck to the pubic bone, which can cause pain.
Stitches
Suspensory
ligament
Repaired
glans clitoris
RECONSTRUCTION
A surgeon can remove or reposition the scar tissue to free the clitoral remnant and bring it to the surface. Some surgeons will also cut the suspensory ligament.
Pubic
bone
Stitches
Suspensory
ligament
Clitoral
remnant
Cut
Scar
tissue
Clitoral
hood
Clitoral
body
Repaired
glans clitoris
Glans
clitoris
Urethra
RECONSTRUCTION
A surgeon can remove or reposition scar tissue to free the clitoral remnant and bring it to the surface. Some surgeons will also cut the suspensory ligament.
SCAR TISSUE
As it heals, the clitoral remnant can become buried by scar tissue and stuck to the pubic bone, which can cause pain.
GENITAL CUTTING
Several types of female genital cutting include the removal or cutting of the glans clitoris, the visible or palpable tip of the clitoris.
Post-surgical complications, like blood clots and fever, were experienced by 155 women, 108 of whom required brief re-hospitalization. Longer-range results were assessed in a one-year checkup, which less than a third of the patients attended. Most reported “improvement, or at least no worsening, in pain and clitoral pleasure.” Sexual satisfaction varied. About a third of women who had never had orgasms reported experiencing them to some degree. But a few who already had regular orgasms reported less sexual satisfaction.
Dr. Foldès said results had since improved, with re-hospitalizations rare and more women reporting positive outcomes. New data has not yet been published.
Dr. Marci L. Bowers, a pelvic and gynecologic surgeon in Burlingame, Calif., visited Dr. Foldès and uses a similar technique, which she says she has performed on over 500 patients.
She said she was asked to learn clitoral restoration in 2007 by Clitoraid, an organization that helps provide the operation in various countries as part of a religion, the Raëlian Movement. The group’s website, which promotes fund-raising programs like Adopt a Clitoris, says one of the movement’s principles is that humans were created by aliens from another planet: “Our body is their masterpiece and the pleasure we feel from it has a purpose.”
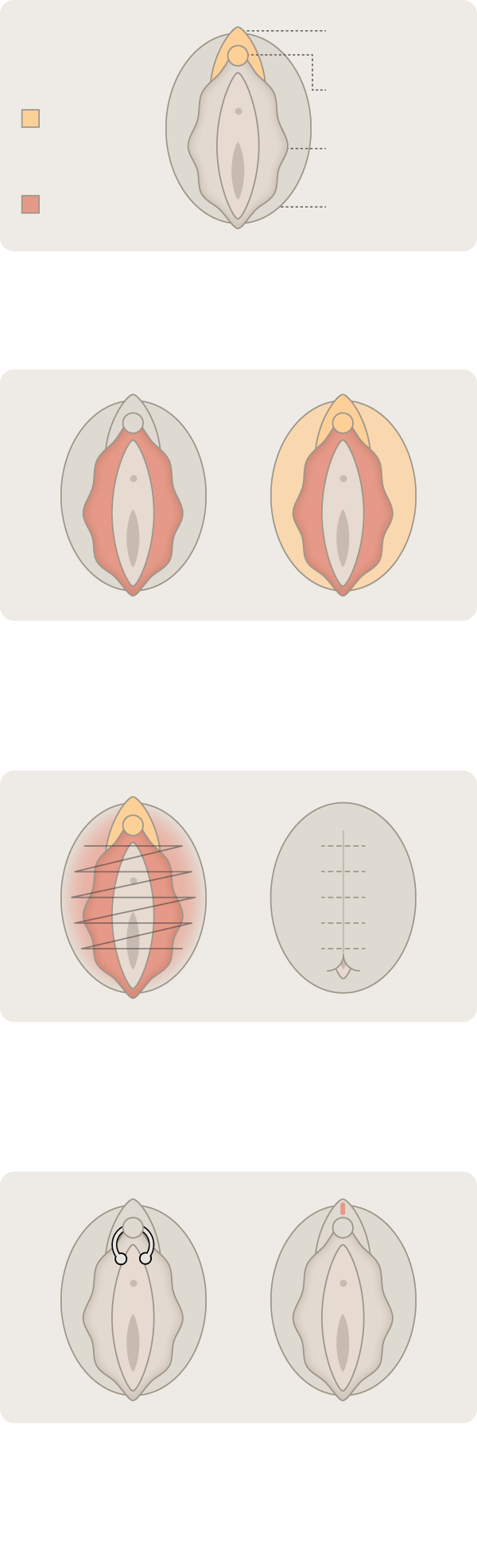
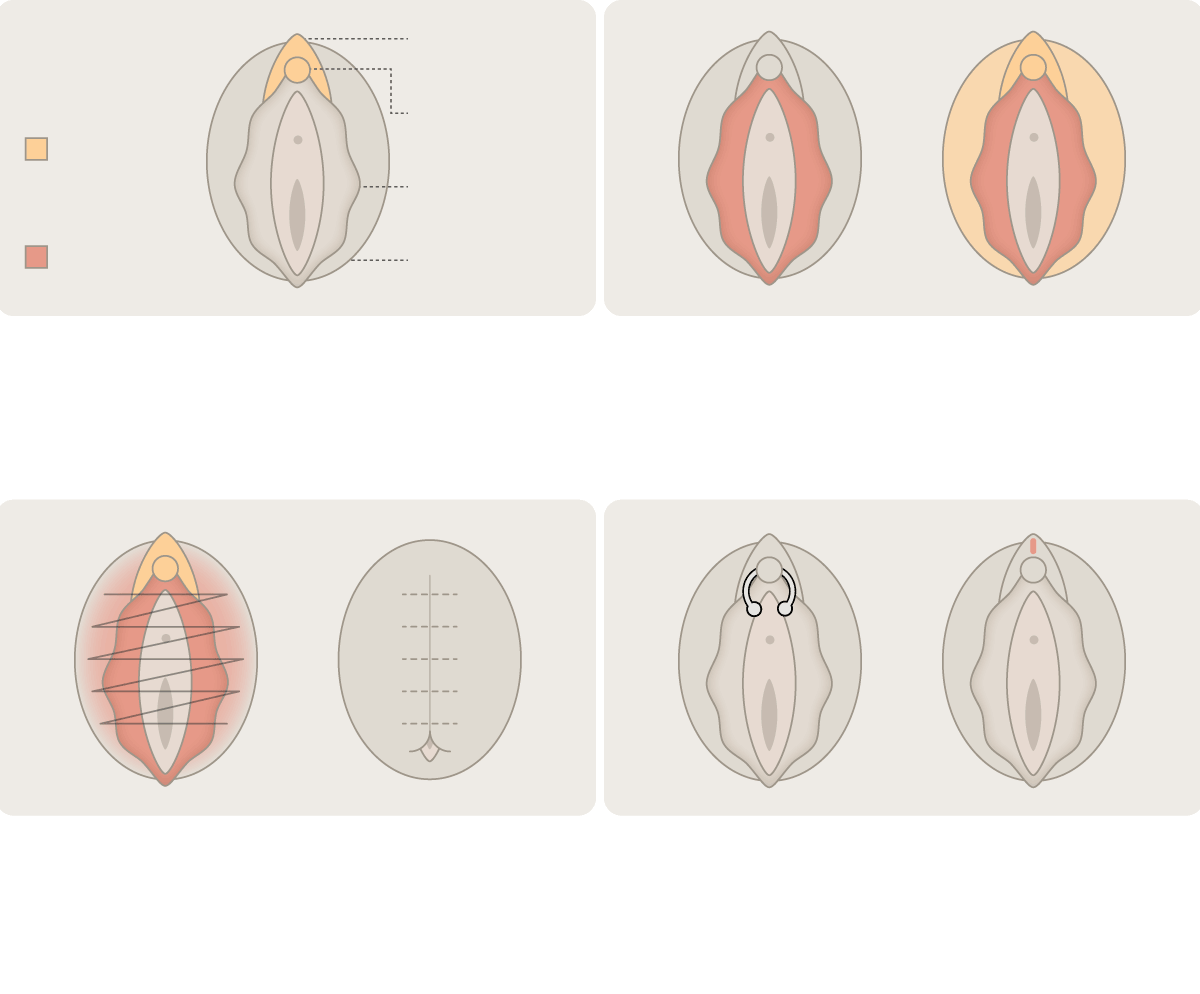
Types of Genital Cutting
The World Health Organization classifies four broad types of female genital cutting or mutilation.
Clitoral hood
Clitoris
Possible
cutting
Labia minora
Cutting
Labia majora
TYPE I (Clitoridectomy)
Partial or total removal of the clitoris or the clitoral hood, or both.
TYPE II (Excision)
Partial or total removal of the labia minora. More severe forms might also remove the clitoris, clitoral hood or labia majora.
TYPE III (Infibulation)
Narrowing and covering the vaginal opening by cutting and fusing the labia minora or majora. May also include cutting the clitoris and hood.
TYPE IV
Other harmful or nonmedical procedures, including piercing, pricking, incising, scraping and cauterization.
Clitoral hood
Clitoris
Possible
cutting
Labia minora
Cutting
Labia majora
TYPE I (Clitoridectomy)
Partial or total removal of the clitoris or the clitoral hood, or both.
TYPE II (Excision)
Partial or total removal of the labia minora. More severe forms might also remove the clitoris, clitoral hood or labia majora.
TYPE III (Infibulation)
Narrowing and covering the vaginal opening by cutting and fusing the labia minora or majora. May also include cutting the clitoris and hood.
TYPE IV
Other harmful or nonmedical procedures, including piercing, pricking, incising, scraping and cauterization.
Dr. Bowers, a transgender woman who has long performed genital reassignment surgery, says that while she is Clitoraid’s lead surgeon, she is not Raëlian. She described the religion’s founder, Claude Vorilhon, called Raël, by saying, “If the Man from Glad and George Jetson had a love child, this is the guy.”
“Their organization is controversial, but the goodness is there,” Dr. Bowers said about Clitoraid, which refers some patients to her California clinic, where she has a yearlong waiting list for clitoral restoration.
Dr. Bowers said that initially she did not always fully detach the suspensory ligament, and “I had quite a number of patients where the clitoris just retracted.” Now, she said, complications are rare, besides a few infections.
About a third have emerged from surgery with an intact clitoris “like a pea in a pod,” and pain has been eased for patients whose constricted vaginal openings were previously “tearing and retearing during sex,” she said.
“We get anecdotal nice stories of people having their first orgasm,” Dr. Bowers said. But, she added, some patients said their sexual enjoyment did not improve, and others reported “a sensation, but not the sensation.”
Some experts are much more cautious about recommending or performing clitoral reconstruction. Dr. Jasmine Abdulcadir, an obstetrician-gynecologist at Geneva University Hospitals in Switzerland, trained with Dr. Foldès, but said she had agreed to requests for clitoral surgery for only about 15 women.
She is a co-author of a review of clitoral reconstruction studies that concluded more evidence of safety and efficacy was needed.
“Why do women have to be considered incomplete or sexually deprived?” she said. “Maybe the woman already has orgasms. She doesn’t have pain, but she wants the surgery to feel more like a woman.” Unless women are in pain, Dr. Abdulcadir requires they wait three months and undergo counseling and psychosexual therapy. After that, she said, less than a fifth choose surgery.
Dr. Nour, at Brigham and Women’s Hospital, also prefers counseling over surgery, noting that “sexuality is so complicated.” She has referred a few patients to Dr. Foldès, but worries about nerve damage from surgery and discomfort from a resurfaced clitoris.
She said she would consider supporting surgery for women who undergo counseling, understand the safety and efficacy risks and strongly believe they need reconstruction to feel complete. “If data clearly demonstrates that clitoral reconstruction is the best method, I’d be the first person to tell everyone to do it,” she said.
A learning curve for surgeons and patients
Marian Gbaya’s experience shows that there is still much to learn about surgical methods and patients’ desires.
Ms. Gbaya, now 27, initially accepted what she was told as a girl in Sierra Leone: that if her clitoris was not severed, she might become sexually promiscuous and men would think “you’re walking around with the dirty stuff that needs to be cut.”
But at 20, soon after joining her mother and sisters in Columbus, Ohio, she began seeing things differently. At a Job Corps program, she heard young women discussing sex, mentioning the clitoris. “How come you still have that?” Ms. Gbaya says she wondered, keeping quiet because she had been told in Sierra Leone that if she disclosed her cutting “you will die.”
Men she dated, she said, reacted harshly to her anatomy: “Can’t deal with that. I’m gone.”
Her solution was to avoid sex. But while studying cosmetology and training in weight lifting, she increasingly felt her body was not whole.
“I do beauty, I’m trying to be a body builder,” she said. “I cannot do that if I’m walking around with an insecurity.”
Describing a 2017 consultation with Ms. Gbaya, Dr. Percec said: “I remember her specifically saying, ‘I don’t care if I lose pleasure. I just want to look normal.’”
Ms. Gbaya’s clitoris and labia minora, the thin rim around the vagina, had been partly cut off. The sulcus, between the clitoris and labia majora, was gone, Dr. Percec said.
Dr. Percec, director of basic science research in plastic surgery at Penn Medicine, has developed her own surgical approach, reusing scar tissue whenever possible, she said. Unlike Dr. Foldès, she does not cut the suspensory ligament, believing that her method better protects nerves and blood vessels.
Yet she is also learning on the job. For example, until she can find a psychologist to help ease women’s post-surgical adjustment, she has started requiring patients to read books about intimacy and sex.
With each of her 11 patients — from Delaware, Maryland, New York, Ohio and Pennsylvania by way of Mali, Niger, Sierra Leone and Sudan, — Dr. Percec has adjusted her method.
When her first patient, Ms. Sillah, remained in pain two weeks post-surgery, Dr. Percec began prescribing women an ointment with lidocaine. When another patient struggled with a dressing, Dr. Percec began sewing on gauze with dissolving stitches. Two patients needed additional surgery, one because her clitoris partially adhered again, possibly because her work uniform included snug pants, Dr. Percec said.
Later, Dr. Percec began grafting fat into the labia, theorizing it would aid healing and add fullness to depleted tissue. She typically takes fat cells from patients’ bellies, but Ms. Gbaya’s muscled body had so little fat that it was taken from the thigh.
Initially, Ms. Gbaya was enthusiastic about the results. She soon returned to the gym and experienced new feelings, she said, as if the clitoris were saying,“Hey, I’m here.” She began a new romance, and said that during sex “I do notice the sensation.”
But eventually, she said, scar tissue formed back over the clitoris. She recently visited Dr. T. Wayne Bloodworth, a cosmetic and gynecologic surgeon who last year opened a nonprofit center in Johns Creek, Ga., that provides free clitoral reconstruction.
Dr. Bloodworth, who trained with Dr. Foldès, said he excised Ms. Gbaya’s re-accumulated scar tissue, cut the suspensory ligament and anchored the clitoris using tiny stitches, steps he considers necessary to keep it from retracting. Ms. Gbaya says she is now “doing great.”
Dr. Percec, whose hospital prevents her from waiving surgery fees, said she understood why Ms. Gbaya, who is uninsured, would go elsewhere.
Had Ms. Gbaya returned for follow-up care, Dr. Percec said she might have prevented scar tissue buildup with a technique she incorporated in 2018: taking skin from inside the cheek and grafting it over the clitoris.
“When you leave it uncovered like I was doing initially, letting it heal on its own, that raw surface can adhere to itself, forming scar tissue,” she said. “With any operation that we design, it’s going to be a work in progress, and it’s going to get better.”
In the operating room
Before her surgery last year, Aminata Welcome, 33, who immigrated from Niger, talked with her preteen daughter, showing her drawings from a medical website.
“I explained to her, ‘This is what a woman’s private part looks like versus someone who went through cutting, mutilation,” Ms. Welcome recalled. “‘As a baby, this happened to me. I’m missing this part. Yours is like this; Mommy’s looks like that.’”
Ms. Welcome, a Philadelphia bus driver who regularly works nights, assured her that “medicine has come up with solutions, and I am getting fixed.”
“Are you going to be O.K.?” her daughter asked.
“Yes,” Ms. Welcome replied, “Mommy’s going to be O.K.”
The morning of her operation, dressed in a black-and-gold abaya, she swept the air with orange-polished fingernails as she described how American men she dated after her divorce dumped her when they learned she had been cut.
“I’ve been rejected three times because of it,” she said. One boyfriend asked if she was transgender. Another told her that “he likes to play with the clitoris, so if I don’t have one, he doesn’t know what he can do with me.”
Heading to the surgery center, Ms. Welcome said, “I’m realistic that it’s never going to be like it never was cut away from me.” She shielded her eyes, praying silently. “This surgery is going to make me feel more like a woman.”
In Operating Room 1, after Ms. Welcome’s anesthesia took effect, Dr. David Colen, the chief plastic surgery resident, scraped tissue from inside her cheek.
“Cheek skin cells are closest to the skin cells over the clitoris,” Dr. Percec explained.
She removed fat from Ms. Welcome’s abdomen with a syringe.
Pressing the scar tissue, she said, “I can feel the clitoral remnant.”
She sliced carefully. “There are 8,000 sensory nerves on the tip of the clitoris, as opposed to the tip of the penis, which has about 4,000,” she said.
“But who’s counting?” Dr. Colen replied.
An hour later, Dr. Percec unearthed about three centimeters of the clitoris. No labia minora remained. Dr. Percec stitched skin “to recreate the rim that was lost,” she said.
The doctors placed the cheek-cell skin graft over the surgical opening and injected fat around it.
After two hours in recovery, Ms. Welcome was discharged. Exhausted, she rested on a green velour sofa at home.
“This is something I’ve been looking for — for the longest,” she said, her voice soft but strengthening. “And here I am.”