As a pelvic health physiotherapist, I considered myself an expert in diastasis recti. After all, I’d been treating the condition for nearly 20 years in my patients.
Then, after my third pregnancy, I diagnosed the condition in myself.
Despite all my education and experience, my first reaction was fear. Because the conventional wisdom for so long has been to go slow to avoid anything that might make the diastasis recti worse, my instinct was to approach the condition conservatively.
I worried.
Would I ever be able to do abdominal training again?
Would I be able to run long distances?
Would yoga no longer be safe?
What about Pilates?
Even for an expert like me, it was hard to figure out what having diastasis meant for my fitness. What exercises could I do? Could I fix the gap in my abdominal muscles? Was I “broken” in some way?
After working with another physiotherapist and a coach I finally began to separate the information from the misinformation about diastasis recti.
 My physiotherapist and my coach helped me realize I wasn’t broken — with diastasis recti, my abdominal muscles simply couldn’t generate as much tension and intra-abdominal pressure as before. They also reminded me that there are still many exercise options available to someone who has diastasis recti.
My physiotherapist and my coach helped me realize I wasn’t broken — with diastasis recti, my abdominal muscles simply couldn’t generate as much tension and intra-abdominal pressure as before. They also reminded me that there are still many exercise options available to someone who has diastasis recti.
Since that experience, I have been able to apply this deeper knowledge and understanding to help other women with diastasis recti feel and move better — without fear or limitation.
Here’s how to help a client with diastasis recti (or yourself) return to exercise safely.
First Things First: What Is Diastasis Recti?
If you or your client is diagnosed with diastasis recti, your first question is probably: what is that?
Here’s a quick explanation:
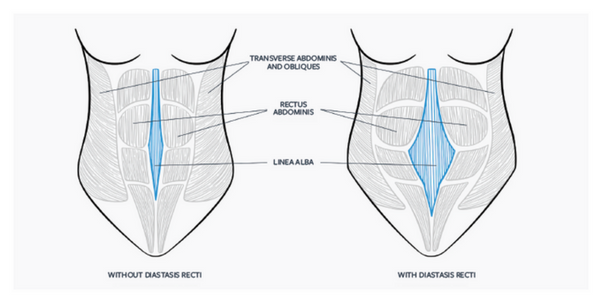
Diastasis recti has been historically defined by “the gap,” or the inter-rectus distance (the distance between the two sides of the abdominis rectus).
During pregnancy, the linea alba — the connective tissue that runs along the midline of the abdomen from the sternum to the pubic bone — softens and becomes more lax. The span of the connective tissue widens, and the rectus abdominis muscle bellies (the right and left sides of this muscle group) move wider apart to allow the abdominal wall to expand as the pregnancy develops.
This natural separation of the abdominal muscles commonly occurs during the third trimester and persists for some time after childbirth.
Most of the research on diastasis recti has been focused on closing the gap, and until recently, the goal of many postpartum exercise programs has also been to reduce or close the gap, as a means of recovery from diastasis recti. In the past, exercises have focused on physically bringing together the two sides of the abdominal muscles (using a band or literally crossing your arms over your abdomen and using your hands to bring both sides of the abdominal muscles together). The idea was to train both sides of the rectus abdominis to work next to each other again.
More recent research is finding that closing the gap is not as important as regaining tension in the linea alba, thus redefining what “healing” diastasis recti means.
Does everyone get diastasis recti during pregnancy?
Almost 100 percent of pregnant women will develop diastasis recti by the third trimester, and pretty much every woman will have a diastasis of greater than 16 millimeters by weeks 35 to 39 of her pregnancy.22 There is no clear way to identify who is most likely to have abdominal separation that persists months after pregnancy.
In the postnatal period, some women’s diastasis recti will “heal” without any intervention (assuming that no additional stress or aggravation of the separation exists). More than half still have a wide separation eight weeks after delivery, and although some recover by six months, many have not recovered at even one year.
A study in Norway found that almost one-third of women still had at least a mild separation at 12 months postpartum (and consequently that two-thirds didn’t — which, according to the study, means that the diastasis recti had “healed”).12
Many women seek help with their diastasis recti because they don’t feel strong and don’t like how their body looks after pregnancy.
Some women with diastasis recti struggle to feel their abdominal muscles in workouts and may tell you their belly feels hollow or disconnected. Sometimes you may notice the belly “cone” or push out through the gap.
You can assess your client’s diastasis recti — and you can teach clients to self-assess.
While ultrasound imaging has become the gold standard for accurate measurement of the inter-rectus distance, finger-width measurement remains the most commonly used screening method in clinical and training environments.
 In this type of assessment, have your client lie supine, ask her to lift her head and shoulders slightly off the ground, and hold that position. You then use your fingers to assess both the gap distance above and below the umbilicus and the ability of the linea alba to create tension across the gap. You will also observe the depth of the gap and monitor your client’s breathing strategies during the slight sit-up movement.
In this type of assessment, have your client lie supine, ask her to lift her head and shoulders slightly off the ground, and hold that position. You then use your fingers to assess both the gap distance above and below the umbilicus and the ability of the linea alba to create tension across the gap. You will also observe the depth of the gap and monitor your client’s breathing strategies during the slight sit-up movement.
The tautness that you can feel — or not — in your client’s tissues can indicate whether there’s good or poor tensioning of the linea alba. Activating the transversus abdominis before and during the maneuver can improve tensioning. To help your client activate her transversus abdominis, cue her to focus on her exhale as she performs the movement.
Can diastasis recti be prevented? Here’s what the research says.
Some of your pregnant clients will want to know how they can prevent diastasis recti or how they can “fix” it or make it go away after pregnancy.
Because there’s so much misinformation about diastasis recti readily available, trainers, coaches, and rehabilitation professionals must understand (and remind their clients) that there’s a lot still unknown.
Diastasis recti research is still very limited compared to other more mainstream concerns such as low back pain. However, it’s a growing area of research, and the quality of that research is steadily improving.
A client may blame herself, believing she actively caused her diastasis recti or is doing the wrong things to address it in postpartum. You may help her go a little easier on herself by explaining that in addition to the lack of evidence-based prevention protocols, one thing emerging from the research is that some factors influencing diastasis recti may not be beyond her control.
For example, one recent study found that the collagen make-up in the linea alba may play a key role in how diastasis recti develops.7 Some collagen types may not be as supportive or elastic, which can potentially influence depth and gap distance or the abdominal muscles’ ability to manage intra-abdominal pressure.
Additionally, factors such as your client’s gender, the presence of a hernia, her history of abdominal surgery or C-section, the number of pregnancies and births she’s had, and the condition of her skin all may potentially play a role her diastasis recti diagnosis.1
Many commercial training programs focus on strategies to control activity-related intra-abdominal pressure before and during pregnancy — including the Valsalva maneuver with weight lifting and chronic straining with toileting. However, these programs and strategies need further research to show their efficacy in preventing DRA.
Being diagnosed with diastasis recti can be stressful and confusing. Luckily, as a coach, you’re in an excellent position to help your clients return to exercise safely, while also feeling strong, healthy, and empowered.
Here are five ways you can help.
1. Dispel myths and reduce fear.
Myths about diastasis recti abound, and some of your clients may tell you they feel broken. Clients who feel scared and avoid exercise will continue to lose strength. You’re in a great position to help them.
Your client may have read or heard myths such as:
- That diastasis recti is preventable (it’s not!)
- That if she doesn’t have it after her first delivery, she won’t have it later (that’s not the case).
- That diastasis recti only occurs after pregnancy (in fact, it’s present in almost every pregnancy by the third trimester — it’s just harder to notice because the pregnancy makes the abdomen firm and the skin pulls taut over the belly.)
First and foremost, reassure a client with diastasis recti that she is not broken. Use your coaching expertise not only to help her focus on reestablishing efficient control of intra-abdominal pressure and improving abdominal strength, but also to help her feel strong and confident in her body again.
2. Provide realistic, progressive exercise programs.
Your client’s post-pregnancy training should focus on helping her regain strength and confidence in her body. With evidence-based program design and good, ongoing communication, you can help your postpartum clients achieve these goals.
Should clients with diastasis recti avoid certain exercises?
 Increasingly, it seems like no exercise is off limits, across the board, for all women with diastasis recti.
Increasingly, it seems like no exercise is off limits, across the board, for all women with diastasis recti.
The more we learn about diastasis recti and the factors involved, and the more we see many women continue to participate in challenging sports and activities without worsening symptoms, the more encouraging — and necessary— it becomes to keep looking for new and better answers.
As research and evidence continue to progress, there are now fewer limitations on the types of exercise women with diastasis recti can do.
That said…
We recommend avoiding the following categories of exercise in early postpartum (when she is least likely to be able to control intra-abdominal pressure effectively):
- Advanced abdominal exercises that put a lot of stress on the abdominal wall
- Plyometric exercises
- Intense exercises or exercise classes
Advanced Abdominal Exercises
This category includes the abdominal exercises we believe should be avoided in early post-pregnancy and possibly added to the later stages of a postnatal rehabilitation program:
- Exercises in which the belly/lower pelvic region is bulging up or out (e.g., crunches and sit-ups, leg raises, bicycles, knee tucks, jackknives).
- Exercises in which the belly is hanging down toward the floor and the hands are a farther distance from the feet or knees (e.g., front planks and variations, pushups, renegade rows).
This is not to say that these exercises are “bad” and must always be avoided, but in our experience, postnatal women should gradually progress toward these exercises, rather than start with them. Make sure that you avoid exercises that cause the abdominal wall to bulge outward (especially at the midline), cause any stress to her C-section incision, or cause leaking of urine.
In exercises where the belly may be hanging toward the floor, your client may feel like her insides are “spilling out” of her belly if she can’t feel tension in her abdominals. For example, if she’s doing a front plank directly on the floor and she never feels it in her abs, but she feels a ton of tension in her shoulders and upper back or some discomfort in her lower back, you should modify the exercise. Try a different variation, such as the incline front plank or a regression to a hands-and-knees position.
What the research says about abdominal exercises…
Recent research has compared the effect of the curl-up and the drawing-in maneuvers on gap “closure.” (The drawing-in maneuver is typically considered a contraction of the transverse abdominals, the deepest of the abdominal muscles.) Several studies have noted that the curl-up maneuver reduces inter-rectus distance and the drawing-in maneuver increases it.2,6,11,13,15,16
It’s easy to see how things can get confusing, right?
So, are crunches OK then? And if avoiding exercises that could increase the gap or prevent it from healing is one of the biggest concerns for people with diastasis recti, what should we do about deep abdominal training? What about rotation exercises and exercises that train the obliques?
Another study identified that compared to women without diastasis recti, women with diastasis recti “demonstrated significantly lower trunk muscle rotation torque and scored lower on the sit-up test.”3 In the context of the idea that there’s less ability to translate forces across, with the understanding that a larger gap or un-tensioned linea alba has a decreased ability to translate forces,13 it makes sense that trunk muscle rotation torque would be diminished.
No research specifically states that crossover crunches, bicycle crunches, planks, or sit-ups are bad and should be avoided at all costs.
Plyometric Exercises
These include:
- Running, sprinting, jogging
- Jumping, box jump, jumping rope
- Burpees, squat thrusts, and other similar conditioning exercises
Your postnatal client may not yet have sufficient abdominal muscle or pelvic floor muscle strength and coordination to control intra-abdominal pressure as well as support the internal organs.
If her body isn’t quite ready yet, she could be setting herself up for issues such as pelvic organ prolapse, urinary incontinence, or low back and pelvic pain.
Intense Exercises
Your client’s body has experienced some major changes over the past nine months. Now it’s important to re-train it, which requires taking just a couple of steps back to teach the core and pelvic floor muscles how to function at their best again.
Keep your sights on the long-term gains, and encourage your clients to do the same. If a client wants to jump right back into heavy resistance training or abdominal and plyometric exercises, intense cardiovascular workouts, or something like a typical “mom and baby bootcamp” class (with lots of running, jumping, crunches, etc.), she could be risking injury or long-term pelvic floor dysfunction.
It’s your job to explain why those options may not be best for her right now, and to help her exercise in a way that helps her achieve those goals over time.
Explain to your client that it’s more effective to stick to exercises and a workout schedule that will rebuild her strength slowly and steadily, rather than hold steadfast to an idea of where she “should” be or where she left off before pregnancy. The idea is to help your clients be able to continue exercising and enjoying their activity over the long term, with minimal risk for injury and burnout.
Whose Decision Is It?
At the end of the day, it’s important to remember that your client has full autonomy over her body and her decisions.
Sometimes, a client may have symptoms and be OK with that. While you can warn her that continuing what she’s doing could make her condition worse, remember that she’s the one in charge of deciding — your role there is to educate her. Make sure to document that you have made an explicit recommendation.
Remember… every client’s postpartum healing experience is different.
Proceed cautiously as your client progresses beyond early postpartum and can start doing more challenging movements. Monitor her diastasis, try different exercises, and scale the workouts based on what you observe and how she tells you she’s feeling.
There are many breathing strategies that may work for your client, depending on the exercise, load, position, and even the day. You can recommend she exhale on exertion, inhale on exertion, hold her breath gently during exertion, exhale slightly right before exertion and hold her breath for the remainder of exertion. Experiment to find what works best for your client in the moment.
Collaborate with a physiotherapist or rehabilitation professional skilled in rehabilitative ultrasound imaging. Find practitioners who use imaging to help their patients improve muscle activation strategies and learn how to use their breath to assist in abdominal activation in different contexts.
If you choose not to program certain exercises with your client, try to use supportive language to explain your choice rather than language that evokes fear. Avoid catastrophizing how they’re feeling or what their body is doing as they perform exercises.
3. Be aware of warning signs.
To help your client heal and continue to make progress, be on the lookout for symptoms that could indicate potential or existing pelvic dysfunction. Always encourage her to listen to her body and trust the signals her body is sending.
When to Proceed With Caution
Abdominal doming or coning is often mentioned in articles about pre- and postnatal exercise, cited as something to be avoided, an indicator that an exercise is too challenging and may lead to negative consequences. But so far, the research hasn’t concluded that doming is harmful.
 Uncontrolled outward pressure forming a central dome or cone on your client’s abdomen, which is not a danger, but can be a potential indicator that she’s not able to control intra-abdominal pressure efficiently, or that an exercise may need to be scaled down. You can help your client test different breathing strategies — including the core-pelvic floor connection breath — and find what works for her in that exercise on that day.
Uncontrolled outward pressure forming a central dome or cone on your client’s abdomen, which is not a danger, but can be a potential indicator that she’s not able to control intra-abdominal pressure efficiently, or that an exercise may need to be scaled down. You can help your client test different breathing strategies — including the core-pelvic floor connection breath — and find what works for her in that exercise on that day.
Planks, crunches, and other high-load exercises in a front-loading position often cause doming, but so can simple dumbbell exercises. You can monitor your client’s abdominal wall and adjust or remove exercises if you notice doming along her linea alba.
When to Stop Exercise and Refer Out
If something doesn’t feel right during an exercise, it’s probably not. If your client just “knows” that what she’s feeling in her body isn’t comfortable, have her stop.
Sometimes exercises will feel a bit awkward after pregnancy, and that’s OK. As a reminder, your client should stop an exercise if:
- It is causing her any pain.
- There’s a pulling sensation through a C-section scar.
- She feels pressure in her bladder or rectum.
- She’s leaking urine during or after a workout.
- She can’t breathe easily.
Remember: regain function first, before doing any intense exercise.
Diastasis recti is not directly correlated with low back pain, pelvic organ prolapse, or incontinence. However, postpartum women often experience one or more of these conditions, and though they may be common, they’re certainly not ideal. Always be on the lookout for these symptoms, and make sure your client follows up with her doctor if she’s experiencing any of them.
Pressure or a feeling of heaviness at the perineum may indicate pelvic organ prolapse, requiring an assessment from OB-GYN or physiotherapist. Pain in the abdomen, pelvis or perineum are not common with diastasis recti and require medical assessment as well.
4. Cultivate a referral network.
If you have a referral network, you’ll always have support from a team of health professionals.
Postpartum women may work with various healthcare professionals of different disciplines, and understanding what each professional does is very important, so you know when to refer your client to another professional.
For example, a physiotherapist trained to work with athletes and active individuals who have diastasis recti can work with your client to identify strategies that help her improve intra-abdominal pressure control.
One thing: make sure you’re all on the same page with the message that having diastasis recti doesn’t mean your client has to stop movement altogether.
5. Practice compassion.
Be sensitive and compassionate with your clients and recognize that everyone is different.
 For many women, their postpartum body may feel foreign, and in many cases, they may be looking for the quickest way back to how they looked and felt before pregnancy.
For many women, their postpartum body may feel foreign, and in many cases, they may be looking for the quickest way back to how they looked and felt before pregnancy.
Your clients’ expectations may range from acceptance of the changes they’re experiencing to complete rejection of a body that rose to the enormous challenge of growing a small human in nine months. Social media has intensified postpartum messaging, causing many women to feel inadequate or implying they’re to blame for the separation of their abdominal muscles.
Harness this opportunity to re-examine your beliefs about diastasis recti, to work collaboratively with your clients to understand their fears regarding exercise and movement, and to provide reliable evidence-based guidance as they work to heal, regain strength, and feel good in their own skin again.
If you’re a health, fitness, or nutrition professional (or you want to be)…
Learning how to coach your pre- and postnatal clients, patients, friends, or family members so that they can feel healthy and strong through pregnancy and beyond is both an art and a science.
If you’d like to learn more about both, consider enrolling in our Pre- and Postnatal Coaching Certification, which opens for enrollment VERY soon.
Our Pre- and Postnatal Coaching Certification is the most respected coaching certification in the world for working with pregnant and postpartum women
If you’re like most of the folks who enroll in our certification, you’re probably aware — maybe from personal experience — there’s a serious gap in high-quality, well-vetted, up-to-date information about helping pre- and postnatal women.
And that’s precisely why we created our Pre- & Postnatal Coaching Certification.
This certification gives health, fitness, and nutrition professionals — and aspiring professionals — the skillset, knowledge, and toolkit they need to successfully and confidently coach pregnant and postpartum women.
Our Coaching and Training Women Academy has certified thousands of professionals in 70+ countries around the world. Their results have been astonishing.
Now, we’re offering all that knowledge and training to you.
Interested? Add your name to our no-obligation pre-sale list. You’ll save up to 33% and secure your spots 24-48 hours before the public.
On September 3rd, 2019 we’re opening enrollment to our Pre- and Postnatal Coaching Certification to a limited number of students.
To learn more, check out our pre-sale list which gives you two huge advantages:
- You’ll pay less than everyone else. The students who are most eager to level up their coaching skills are our most successful students, so we like to reward those who join the pre-sale list by offering a discount of up to 33% off the general price.
- You’ll get to enroll early. We only open enrollment twice per year, and spots always sell out FAST. By joining the pre-sale list, you have the chance to enroll 24-48 hours before the general public, increasing your chances of getting a spot.
If you’re ready to learn exactly how to keep your pre- and postnatal clients and patients safe, healthy, and strong, during and after pregnancy…
This is your chance to enroll in the world’s most respected Pre- and Postnatal Coaching Certification.